The fluorescent lights of the underground hospital garage hummed with a low, agonizing buzz that seemed to vibrate inside Dr. Marcus Thorne’s skull. It was 11:32 p.m. The air was thick with the scent of sterile latex and old engine oil. Marcus’s hands, the same hands that had spent the last fourteen hours delicately suturing an ascending aortic aneurysm, were now trembling. Not from exhaustion, but from the raw, cold adrenaline of staring down the barrel of a Glock 17.
“Hands up! Get on the ground! Now!”
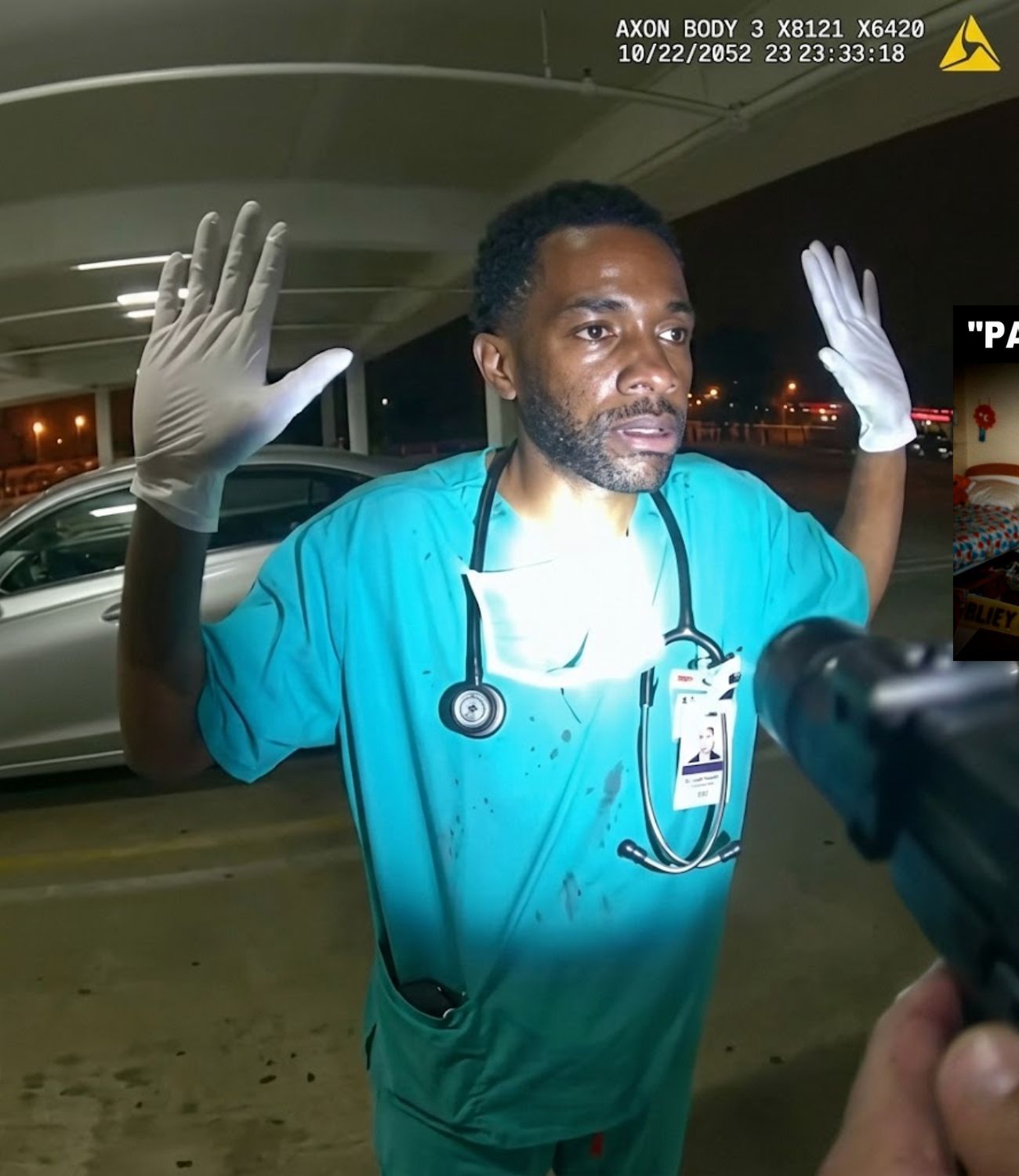
The shout tore through the silence of the concrete tomb. Marcus froze. He was still in his blue surgical scrubs, his white clogs stained with a single drop of blood from a patient he had just brought back from the brink of death.
“I’m a trauma surgeon,” Marcus said, his voice a practiced anchor of calm, though his heart hammered against his ribs like a trapped bird. “I just left the OR. My badge is on my chest. Do not reach. I’m complying.”
“Get face down on the concrete! Do it now or I will fire!”
The officer’s eyes were wide, white-rimmed with a terrifying mix of fear and unchecked authority. The metal slide of the handgun caught the overhead light, a silver glint that promised a permanent end to a life dedicated to healing. Above them, in the hospital tower, families were weeping with joy because Marcus had saved their loved ones. Down here, Marcus was just a black man in a dark garage, and to the man behind the trigger, that was enough to constitute a death sentence.
“Call hospital security,” Marcus pleaded, slowly lowering his knees to the cold, grime-slicked floor. “They know me. I work here.”
“Shut up! Face down!”
The click of the safety being disengaged echoed like a gunshot in the confined space. Marcus felt the bite of the concrete against his cheek. He closed his eyes, the smell of disinfectant on his sleeves a cruel reminder of the life he was about to lose. In the distance, an elevator bell chimed—a mundane, cheerful sound that signaled the world was moving on, oblivious to the fact that a healer was being treated like a Tier-1 predator.
The garage was almost empty when he heard the shout.
“Hey! Stop right there!”
He froze.
“I’m just getting to my car.”
“Hands up now!”
It was 11:32 p.m. beneath a hospital tower still glowing with late-night activity. Fluorescent lights buzzed overhead, casting hard reflections off concrete pillars. The smell of disinfectant clung to his scrubs, a reminder of the operating room he had just left after fourteen hours without daylight. A black man in surgical shoes stood between parked cars, keys in one hand, exhaustion heavy in his shoulders.
“Don’t move!” the officer yelled. “Get on the ground!”
The surgeon slowly raised his hands, palms open, fingers spread. His badge hung from his neck, swinging slightly with his breath.
“I’m a doctor,” he said. “I just finished surgery.”
The officer did not lower his weapon. In fact, he raised it higher, arms locked, barrel steady.
“I said, get on the ground.”
The surgeon’s heart began to pound harder than it ever had during an operation. He had guided hands through open chests; he had stopped bleeding with calm precision. None of that training applied here.
“I work here,” he said again, voice controlled but tight. “My ID is right here. Do not reach.”
The officer snapped. The space between them felt impossibly short. Concrete amplified every sound: the click of the safety, the echo of a distant elevator. Somewhere above them, a gurney rolled across tile. The surgeon knelt slowly, careful, one knee touching the cold floor of the garage. His hands stayed raised, trembling now despite his effort. The gun followed him down, never wavering.
“This is a hospital,” he said. “You can call security. They know me.”
The officer’s eyes flicked to the badge, then back to the surgeon’s face. His jaw tightened.
“Why are you down here this late?”
“Because people don’t stop bleeding at 5:00,” the surgeon replied.
A car door slammed on the far side of the garage. Footsteps paused. Someone whispered.
“What’s going on?”
The officer shouted again, louder, sharper, as if volume could justify what was happening.
“Face down!”
The surgeon lowered himself further, cheek pressed against concrete that smelled faintly of oil. His pulse roared in his ears. He thought of the patient he had just closed, of the family waiting upstairs, of how easily a night meant to save a life could end his own. What should have been a quiet walk to his car after saving someone else had turned into a moment balanced on a trigger. And in that underground garage, with a gun trained on his back, the difference between healer and threat had been decided in seconds—without evidence, without question, and without mercy.
Long before the garage and the drawn weapon, his life had been shaped by discipline, not fear. He had chosen surgery knowing exactly what it demanded: years of training that blurred together, nights spent memorizing anatomy while friends slept, residency that taught him how to function when exhaustion hollowed out everything else. He learned to steady his hands when a life depended on it, to slow his breathing when alarms screamed, to make decisions that could not be undone.
He earned his place in that hospital the hard way. Fellowships, board certifications, countless hours under fluorescent lights brighter than the ones in that garage. Patients trusted him with their bodies; families trusted him with their futures. He carried that weight quietly, without ceremony.
That night’s surgery had been complicated. Unexpected bleeding—a moment where the room went silent except for monitors and controlled voices. He stayed focused. He always did. When it was over, he scrubbed out slowly, muscles aching, mind still replaying every step the way surgeons did when they cared enough to doubt themselves. He left the operating floor wearing the same scrubs he had put on before dawn, badge clipped where it always was, phone buzzing with messages he ignored for later. His only thought was getting home, sleeping, then coming back to do it again.
The officer had arrived with a different mindset. He was assigned to patrol the hospital area after a recent string of car break-ins nearby. Briefing notes emphasized vigilance, late hours, unfamiliar faces. The garage was listed as a soft spot: concrete levels, limited visibility, echoes that made every movement feel closer than it was. His record showed confidence under pressure, quick reactions, and a tendency to escalate early to maintain control. Prior complaints about aggressive posture had been reviewed and closed—no injury, no discharge, no sustained finding.
That night, when he saw a black man in scrubs walking alone through the garage, fatigue did not register as exhaustion; it registered as intent. The badge did not register as employment; it registered as something to be questioned. When the man spoke calmly, explaining who he was, it did not lower the officer’s guard; it raised it. Calm was read as practiced professionalism, as deception. The space filled with imagined threat instead of evidence.
Two men stood in the same garage, both sworn in different ways to preserve life. One had just saved it with his hands; the other believed he was protecting it with a gun. They met not because of chance, but because assumptions move faster than verification when fear is given authority. And once that fear took control, the surgeon’s years of training, service, and sacrifice meant nothing in the seconds that followed.
The garage began to fill not with people, but with pressure.
“Stay down,” the officer ordered again, his voice echoing off concrete walls. “Do not move your hands.”
The surgeon lay still, cheek against the floor, eyes fixed on the dark line of oil staining the cement inches from his face. His palms were open, fingers spread so far they burned. He controlled his breathing the way he had in operating rooms when a patient crashed. Slow in, slower out. Any sudden motion here felt lethal.
“My badge is on my chest,” he said. His voice came out measured, clinical. “You can see it without me moving.”
The officer did not look. The gun stayed trained on the center of his back.
“Keep talking and I will escalate.”
“Escalate to what?” the surgeon asked quietly. “I am already on the ground.”
The question went unanswered. Footsteps approached from the far end of the garage. Two nurses froze near an elevator bank, hands covering their mouths. A security guard leaned out from behind a parked SUV, radio halfway to his shoulder, eyes locked on the weapon.
“What’s happening?” the guard called out.
“Police business,” the officer snapped without turning. “Stay back!”
The guard hesitated.
“That’s a doctor. He just came off shift.”
The officer’s grip tightened.
“No one asked you!”
The surgeon felt the gun move slightly as the officer adjusted his stance. The barrel traced his spine, settling again. His heart pounded so hard it blurred sound at the edges. He thought of the precision he demanded of himself in surgery. Millimeters mattered. Steady hands mattered. Here, his life depended entirely on someone else’s restraint.
“I am not armed,” the surgeon said. “I have not committed a crime. This is a hospital employee garage with cameras everywhere.”
The officer laughed once, sharp and humorless.
“Cameras don’t stop bullets.”
More people had gathered now. A resident, a janitor pushing a cart, phones lifted—not hidden anymore. The garage lights reflected off lenses, tiny witnesses capturing every angle. The officer noticed them and raised his voice, commanding the space. Everyone stepped back now. No one moved fast enough to satisfy him.
The surgeon felt something new settle in. Not panic, but awareness that this was no longer about safety. It was about control—about whether the man holding the gun could lower it without losing authority in front of witnesses. And the longer it went on, the harder that became. He pressed his forehead to the floor, not in surrender, but in strategy. Stillness was survival. Silence was calculation.
Above him, the gun remained pointed. Below him, the concrete stayed cold. Between those two realities, time stretched thin, each second a reminder that in this garage, evidence meant nothing, credentials meant nothing, and saving lives hours earlier offered no protection at all. All that mattered was whether fear would loosen its grip before someone pulled the trigger.
The gun never wavered, and that was the most dangerous part. Minutes passed without count. The officer shifted his feet, adjusting his stance, but the barrel stayed trained on the surgeon’s back. The fluorescent lights hummed overhead, flickering once briefly as if even the garage hesitated.
“Do not move,” the officer said again.
The surgeon did not answer. His breathing stayed controlled, shallow enough not to rock his shoulders. He knew how quickly a twitch could be misread. He knew how narratives were written after the fact. This was the injustice—not a stop, not a question, but a sustained threat; a drawn weapon held on an unarmed man who had already complied, already identified himself, already surrendered every possible gesture of safety.
The officer took a step closer. The shadow of his arm stretched across the concrete, cutting through the harsh light. The surgeon felt the presence more than he heard it. The weight of it pressed into his spine.
“You give me one reason,” the officer muttered, voice low now, close.
“One reason for what?” the surgeon asked quietly.
“To exist here.”
The words landed, and for a moment, the garage went silent except for the distant whir of an elevator motor. No one moved. No one breathed loudly. The nurses near the wall held their phones steady, eyes wide, faces pale.
The security guard tried again, calmer this time.
“Officer, this is a hospital surgeon. We can verify him right now. There’s no threat.”
The officer snapped his head toward the guard, gun still pointed downward.
“I didn’t ask for your assessment!”
He turned back just as quickly, barrel resettling on the surgeon’s body. The surgeon closed his eyes for a fraction of a second, then opened them. He focused on staying present, on staying alive. In the operating room, danger was measured and addressed. Here, danger was arbitrary. It depended entirely on whether the man holding the gun could step back without feeling exposed.
The officer’s finger rested along the trigger guard, not squeezing, but not relaxed either—just close enough to make every second count. This was no longer confusion. It was no longer caution. It was force maintained beyond reason. And in that underground garage, where concrete walls trapped every sound and camera lenses watched without intervening, a surgeon who had just saved a life lay face down, waiting for someone else to decide his was worth sparing.
The shift began with a voice the officer could not ignore.
“That’s enough!”
Hospital security arrived first, two officers moving quickly but deliberately, hands visible, radios already raised. One of them recognized the badge on the surgeon’s chest immediately.
“Doctor, don’t move.”
This guard said it not to restrain him, but to protect him.
“We’ve got this.”
The armed officer hesitated. His eyes flicked between the security uniforms, the phones still recording, and the surgeon on the ground who had not moved an inch.
“This individual matched a description,” the officer said, the words coming out stiff now.
“Description of what?” a security supervisor asked as he stepped into the light. “A surgeon leaving his shift?”
He pointed upward.
“Cameras are on every level. We already checked. He badged in twelve hours ago. He’s scheduled. He’s cleared.”
The officer’s jaw tightened. He did not lower the gun yet. The supervisor held his ground.
“Officer, you need to holster your weapon. Now.”
For a long second, nothing happened. The garage felt like it was holding its breath. Then the gun lowered slowly—not with confidence, but with reluctance. The officer stepped back half a pace and holstered it, the sound loud in the quiet that followed.
“Doctor, you can sit up,” the supervisor said gently.
The surgeon pushed himself up onto his elbows first, then sat back on his heels. His hands shook now that he allowed them to. Blood rushed back into his fingers, tingling, painful. He stayed where he was, eyes level, making no sudden moves.
“I told you who I was,” he said, not angry, just clear. “You never checked.”
The officer looked away. A lieutenant arrived moments later, having been called by security. He took in the scene in seconds: the drawn phones, the surgeon on the floor, the officer standing rigid, suddenly small.
“Is this the physician everyone’s talking about?” the lieutenant asked.
“Yes,” the supervisor replied. “Trauma surgeon on staff. Badge verified. Cleared access.”
The lieutenant exhaled slowly.
“Doctor, I’m sorry for what just happened.”
The surgeon nodded once. He did not accept the apology. He did not reject it. He simply acknowledged that it existed. He stood carefully, legs stiff, scrubs dusted with grime from the floor. A nurse stepped forward and placed a hand on his arm without asking. He let it stay there. As the lieutenant pulled the officer aside, voices dropped. Policies, use of force, body cameras—the words carried even when meant not to.
The surgeon picked up his keys. His hand shook as he did it. He leaned against his car for a moment, grounding himself against the metal. Around him, the garage buzzed again, but differently now. People whispered. Phones kept recording. No one pretended this had been routine. The truth had surfaced not through argument, but through verification that should have come first. And standing there, heart still racing, the surgeon understood something with absolute clarity: if help had not arrived when it did, this story would have ended very differently. And everyone who had watched it unfold knew the same thing.
The response did not wait for daylight. By the time the surgeon reached home, videos from the garage were already circulating—shaky at first, then clearer. The gun drawn. The commands. The man in scrubs face down on concrete. Medical staff shouting that he was a doctor. The moment the weapon finally lowered.
Hospital leadership released a statement before dawn.
“An incident occurred involving one of our physicians. We are cooperating fully. Staff safety is our priority.”
It sounded careful. It sounded late.
The police department had placed the officer on administrative leave that same morning. Badge surrendered. Weapon logged. Body camera footage pulled. Supervisors reviewed it in silence. No raised voices. No debate. The timeline spoke for itself.
Within days, the surgeon filed suit. The complaint was precise: excessive use of force, unlawful detention, threat of deadly force without probable cause, racial profiling, emotional distress, and loss of sense of safety at his own workplace. Each claim was tied to video timestamps and witness statements from hospital employees trained to recognize danger.
Medical associations spoke up next, not politically, but practically. Physicians cannot function under threat. Hospitals cannot be safe when staff fear being mistaken for suspects in their own garages. Letters were sent. Meetings requested. The story moved beyond one night underground.
City attorneys reviewed the case with a different lens—not public relations risk, but liability. Juries did not like guns pointed at unarmed professionals, especially not in hospitals, especially not with cameras running, especially not when the victim had just finished saving a life. Settlement discussions moved quickly.
$8.9 million became the number that ended them. Not symbolic. Calculated. The cost of a drawn weapon where none was justified. The cost of a city failing to control an officer whose fear had been given a trigger.
The officer was terminated shortly after. The notice cited violations of use of force policy, failure to de-escalate, and conduct unbecoming. His prior complaints were re-examined—no longer isolated, no longer ignored. Policy changes followed: mandatory de-escalation training, clearer protocols for hospital environments, and explicit guidance on weapon presentation. All written after the harm had already occurred.
The surgeon returned to work quietly. Same operating room. Same tools. Same stakes. But the garage felt different now. Every footstep echoed longer. Every shadow felt heavier. Colleagues walked him to his car for weeks without saying why. Justice arrived in numbers, documents, and consequences. It did not erase the moment on the concrete. It did not erase the image of a gun where there should have been trust. But it forced the city to acknowledge that this was not a misunderstanding. It was a failure with a price.
What happened in that hospital garage was not a judgment call. It was a violation of force standards. Drawing a firearm is considered a use of deadly force threat. Policy requires an immediate, articulable threat of serious bodily harm before a weapon is presented. An unarmed individual, compliant, identified, in a controlled environment, does not meet that threshold. Once the surgeon was on the ground with hands visible, any remaining justification disappeared. Keeping the gun trained after that point crossed from caution into danger.
This matters because weapons change outcomes even when they are not fired. Neurologically, a drawn gun escalates stress on both sides. It narrows perception. It shortens reaction time. It increases the chance of catastrophic error from a flinch, a misheard word, or a startled movement. In enclosed spaces like parking garages, that risk multiplies. Concrete echoes distort sound. Shadows obscure depth. Every variable argues for restraint, not escalation.
Bias is what filled that gap. The surgeon’s presence was interpreted through fear instead of context. Scrubs became a disguise. Fatigue became suspicion. Calm explanation became manipulation. None of those interpretations were evidence. They were assumptions. And assumptions do not justify lethal force posture.
For civilians, there are limited survival strategies in moments like this: freeze rather than argue; move only when instructed; keep hands visible at all times; narrate movements calmly if allowed; do not reach for identification unless explicitly told to. Prioritize staying alive over being right. Documentation and accountability come later.
For institutions, the responsibility is heavier. Use of force policies are meaningless if they are not enforced. When no shot is fired, drawing a gun is not a neutral act that becomes serious only after discharge. It is the crisis point itself. Officers who cannot de-escalate in controlled environments should not be patrolling them. Hospitals, in particular, demand heightened restraint. They are places where stress already runs high, where lives are routinely on the edge. Turning healers into targets undermines safety far beyond a single incident.
$8.9 million addressed liability. Termination addressed accountability. Policy revisions addressed exposure. None of it changed the fact that a man who saves lives for a living lay face down on concrete, wondering if he would become a statistic himself. That is the lesson this case leaves behind: deadly force does not begin with a shot; it begins with a decision to treat fear as fact and authority as permission. If that decision is not corrected early, the difference between a close call and a funeral can be measured in seconds.
Disclaimer : This content may be created by AI for entertainment purposes. Any resemblance to real persons, events, or places is coincidental.