The heavy military transport truck ground to a sudden halt, kicking up a massive, suffocating cloud of fine red dust that swirled through the humid air of the American compound. The vehicle’s engine idled with a low, mechanical rumble before the driver cut the ignition, leaving only the sound of settling dust and the distant murmurs of the camp. After a brief pause, the heavy iron chains rattled, and the back gate dropped down with a sharp, resonant metal clank that echoed off the wooden walls of the nearby barracks.
A young boy stepped down from the bed of the truck. His movements were agonizingly slow and deliberate, performed as if the very air surrounding him possessed a physical weight that inflicted acute pain upon his fragile frame. He was a mere boy of eighteen years, yet he carried himself with the heavy, broken posture of an old man. He wore a faded, worn German military uniform that hung loosely off his emaciated frame like an oversized shroud draped over a skeleton. Every single breath he drew caught sharply in his throat, raspy and strained, sounding exactly like a thin wire snagging against rusted iron. Two of his ribs were completely fractured; that clinical reality was immediately obvious to anyone trained in trauma.
But as the camp medic stepped forward to begin the standard intake physical examination, he quickly realized that the broken bones were merely the surface layer, the least significant thing contained within this young boy’s damaged body. The extensive bruising scoring his flesh did not match the narrative of a simple transport accident, the profound weight loss did not correspond to the ordinary hunger experienced by troops on the front lines, and the jagged scars lining his skin were entirely distinct from the kind of wounds a standard battlefield inflicts upon a soldier.
Within the secure perimeter of this United States prisoner of war camp, surrounded by standard guards who expected nothing more than the routine processing of paperwork and the execution of daily military administrative protocols, the quiet medical room was about to transform completely. It was on the verge of becoming the exact physical space where an entire hidden narrative of institutional terror collapses into the open light.
A brand-new group of prisoners arrived at the facility in the precise manner that new groups always arrived—carrying heavily tired faces, deep lines of physical exhaustion etched around their eyes, and the same rigid, guarded silence that characterizes men who have surrendered to their fate. The United States soldiers stationed at the processing center had witnessed hundreds of men exactly like them. They had seen endless waves of soldiers captured across the arid expanses of North Africa, the rugged terrain of Italy, and the blood-soaked fields of France, shuffled across vast oceans and endless rail lines, arriving in massive, anonymous waves that eventually blurred together in the minds of the camp administrators.
But this particular eighteen-year-old boy stood apart from the crowd the very moment his boots touched the dirt after stepping down from the transport truck. He did not possess the hardened, calloused look of a seasoned combat veteran. Instead, he looked remarkably like someone who had been violently pulled out of a catastrophic storm and abruptly commanded to stand at attention on a foreign parade ground. His right hand was pressed firmly against his side, his fingers clutching his uniform as if he were desperately trying to hold his own internal organs together. When a nearby American guard barked an order for him to move faster along the processing line, the boy attempted to comply, but his face instantly flashed with a spasm of agony so incredibly sharp and profound that it caused the guard to pause mid-sentence, his voice dropping.
The first question came quickly, cutting through the ambient noise of the processing yard.
“What happened to you?”
The boy provided his answer in short, excessively careful words, selecting his vocabulary with an anxious, defensive precision.
“I fell during transport.”
He paused, drawing a shallow breath.
“The heavy door slammed against me.”
He looked down.
“It was nothing.”
But his physical body told an entirely different, far more honest story. The defensive manner in which he constantly protected his injured chest was far too practiced, far too instinctual to be the result of a recent, accidental bump. The deliberate way he avoided direct eye contact with anyone in authority was far too precise, revealing a deeply ingrained survival mechanism. He had clearly learned through harsh experience that offering the wrong detail could bring immediate physical punishment, and utilizing the incorrect tone of voice could bring something infinitely worse. Recognizing that he was unfit for the standard barracks processing line, the administration sent him directly to the wooden medical building. This decision was not made out of genuine kindness or sudden empathy; it was executed simply as a matter of standard operating procedure.
Inside the medical building, the atmosphere was heavy and stagnant. The air smelled strongly of pungent chemical disinfectant, mixed with the musty, damp scent of old canvas cots and military blankets. A medic gestured toward the simple wooden cot in the corner of the room. The boy sat down with an agonizing slowness, easing his weight onto the canvas as if every single macro-movement cost him a full day of his remaining life. The medic sat opposite him, preparing his intake forms, and began with the standard, basic administrative questions required by the Geneva Convention protocols.
“Name?”
The boy gave a name, his voice tight and formal.
“Age?”
“Eighteen.”
“Unit?”
He provided a specific unit designation, but the words sounded heavily rehearsed, delivered like a memorized script rather than a natural recollection.
“Date and place of capture?”
He explained that he was captured during the intense, chaotic fighting in Western Europe during the final, desperate push of the Allied advance. It was a time when entire military formations were completely collapsing under the pressure, and young, completely untrained replacements were being frantically thrown into the front lines to fill the gaps left by the dead.
The medic nodded, noting the details down, and then asked the one fundamental question that always matters most in clinical practice.
“Where does it hurt?”
The boy pointed a trembling hand toward his ribcage, fighting to keep his voice perfectly steady.
“It hurts to breathe.”
He looked up briefly, then dropped his gaze.
“I can handle it.”
The medic nodded his head slowly, but he did not accept this neat, simplified version of the injury. He had worked in these transit camps long enough to have seen men lie out of stubborn military pride. He had seen men lie out of a deep, paralyzing fear of what might happen to them if they showed vulnerability. And, most importantly, he had seen men lie simply because someone in authority back across the lines told them exactly what to say, word for word, long before they ever reached the safety of a secure prisoner of war camp.
The medic reached forward, extending his hand toward the buttons of the boy’s worn shirt. The moment his hand approached, the boy flinches violently backward. That sudden, involuntary flinch altered the entire psychological atmosphere of the room. This was completely distinct from the normal flinch of a wounded soldier who expects a painful physical touch; this was the unmistakable, deeply ingrained flinch of a human being who genuinely expects severe consequences for being examined.
The medic paused his movement entirely, lowering his hands, and began to speak in a much softer, non-threatening tone. The boy took a long, ragged exhale, his shoulders dropping slightly, and slowly pulled the fabric of his shirt upward. A massive expanse of deep purple bruising bloomed across his exposed ribs. It was not a single, uniform bruise from a recent impact; instead, it consisted of multiple different shades of blue, purple, yellow, and green, resembling a horrific physical calendar of sustained pain.
The medic’s clinical eyes moved slowly downward. The boy’s stomach was severely hollowed out, the skin stretched tight over the underlying skeletal structure. The natural musculature that should belong to an eighteen-year-old youth was completely gone, wasted away by prolonged deprivation. The medic gently instructed the boy to turn, and on his back, he observed marks that could never belong to a simple fall from a transport truck. There were long, thin lines of raised flesh, old scabs crusted over with dried blood, and distinct places where the skin had healed incorrectly, leaving jagged, uneven scars.
The medic said absolutely nothing yet. He simply continued to write notes on his clipboard. The boy watched the precise movement of the pencil across the paper as if the graphite tip itself were a dangerous weapon. Because the boy knew something fundamental that the camp administration did not yet comprehend: a thorough medical examination can expose far more than simple broken bones. It possesses the power to completely expose the dark reality of the past.
To truly understand why this specific medical examination mattered so profoundly, it helps to understand exactly what a United States prisoner of war camp was structurally designed to be. It was intended to function as an efficient, highly predictable bureaucratic machine. The core mandate was simple: receive incoming prisoners, register their legal names and military numbers, assign them to designated wooden barracks, issue standard clothing if their current uniform was unserviceable, schedule regular daily meals, assign individuals to specific work details, and maintain absolute military discipline throughout the compound. On most ordinary days, this entire administrative system ran like clockwork on established routines.
A prisoner typically arrived tired, dirty, and exhausted, but physically stable. He was systematically inspected, thoroughly deloused in the chemical showers, examined by a medical officer, and moved along into the general population. His entire life and wartime experience became condensed into a single, neat line on an official government form. But human bodies do not always fit neatly into bureaucratic forms.
This medic had worked in the military medical corps long enough to easily recognize the vast difference between a soldier who was merely hungry from short-term combat rations and a soldier who was clinically starved over a period of months. Ordinary hunger looks like physical fatigue, dark circles under the eyes, and general irritability. Severe, long-term starvation looks like the physical body actively shutting down its own non-essential systems. And this young boy possessed that distinct, terrifying look of systemic starvation. His eyes appeared far too large for the gaunt contours of his face. His skin had taken on a dull, lifeless color, closely resembling wax that had been left out in the freezing winter air. His hands shook with a slight, uncontrollable tremor whenever he attempted to hold them perfectly still against his lap.
The medic placed the cold metal of his stethoscope against the boy’s chest and listened closely to his lungs. Each breath drawn by the youth was incredibly shallow and rapid. The right side of his chest moved significantly less than the left side during inhalation, indicating a severe restriction of movement. The medic began to tap gently along the line of the ribs, his movements careful, measured, and entirely controlled. The boy instantly clenched his jaw so tightly that the muscles stand out in sharp relief. He was clearly exerting every ounce of his remaining willpower to avoid making a single sound of distress. This absolute restraint provided the medic with another critical clue. Most men experiencing acute physical pain cannot help but gasp or cry out when an injured area is directly palpated. But this particular boy had been intensely trained by harsh circumstances to remain perfectly silent under torment.
The medic turned to his notepad and ordered an immediate X-ray. The boy visibly stiffened at the mention of the word, his eyes widening slightly as if he genuinely expected the large medical machine to somehow accuse him of a crime or expose a hidden secret. While they prepared the diagnostic equipment, the medic continued to speak to him. This was not a formal military interrogation; it was a casual, low-pressure conversation designed to put the patient at ease.
“Where are you from originally?”
“How old were you when you first joined the service?”
“When did you last see your home and family?”
The boy answered each inquiry with the exact same tight, mechanical control.
“I was drafted into the army.”
“I completed my basic training.”
“I fought on the line.”
“I was captured by the Allies.”
Every single statement was factually correct. Every response flowed smoothly from his lips. Yet, everything about his delivery was completely missing the subtle nuances and emotional variations that make a story feel genuinely human. The medic paused, looking up from the equipment, and asked a question that should be entirely simple and straightforward.
“Who treated your injuries after you got hurt?”
The boy hesitated for only a brief second, but that tiny delay represented the very first visible crack in his carefully rehearsed wall of defense.
“Nobody.”
He shifted his weight uncomfortably.
“There was no time.”
He looked away.
“It is fine.”
But the expression on his face conveyed something entirely different. His countenance revealed that he had deeply learned that physical pain is never a valid reason to receive help. His expressions showed that he had lived through an environment where injuries make you an immediate target for further aggression, rather than a patient deserving of care. And that is the exact moment when the medic begins to strongly suspect that these broken ribs are not the result of a recent transport injury at all. They are the direct physical consequence of something that occurred long before his capture—something close, something intimate, and something deeply personal.
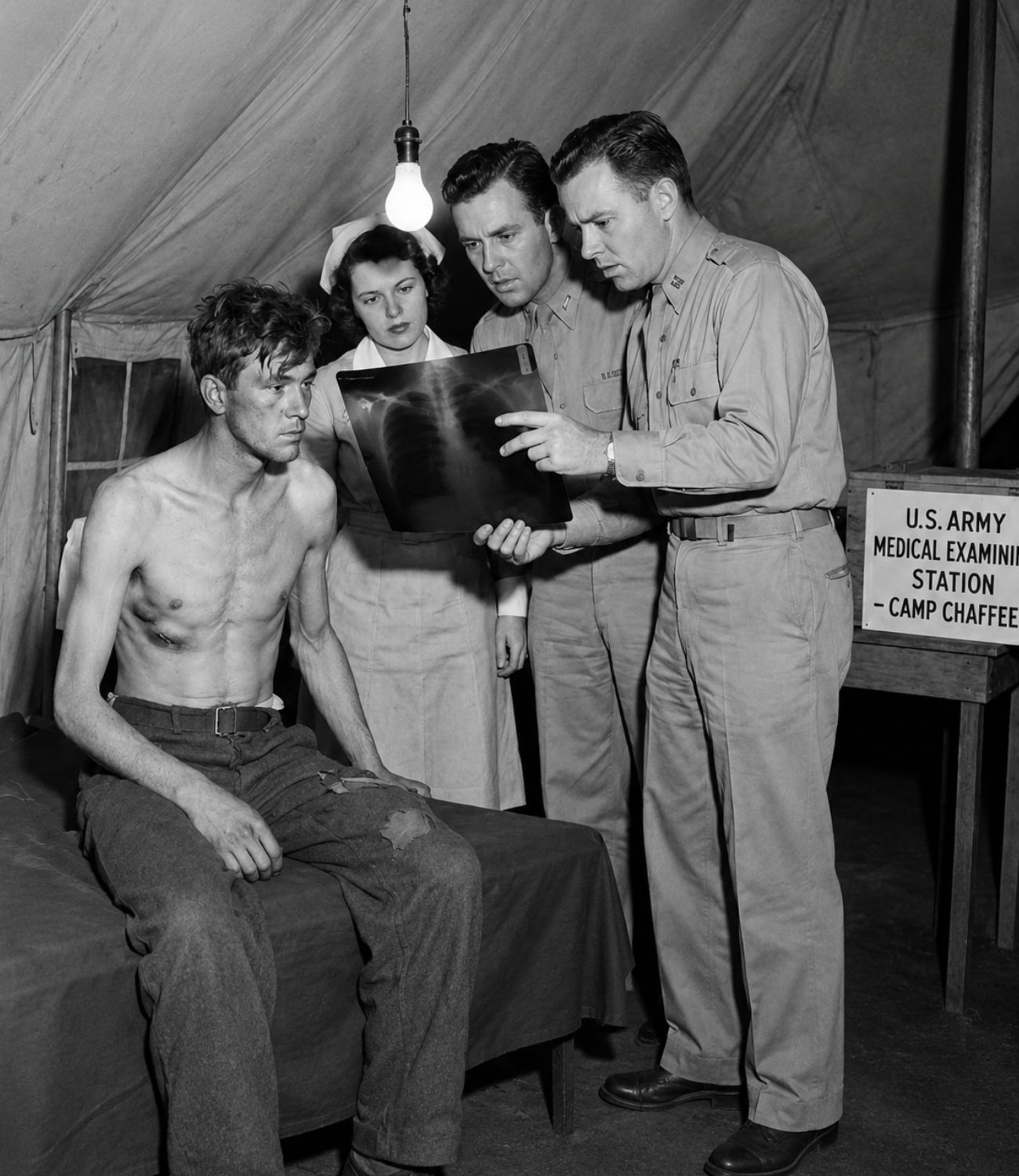
The X-ray room was small, cold, and entirely stark, stripped of any comfort. The boy stood exactly where he was told to stand by the technician. He slowly raised his emaciated arms above his head, his face contorting into a sharp wince as the movement pulled at his damaged torso. The heavy machine emitted a loud, mechanical click as it captured the image. The medic stood nearby, watching his breathing patterns closely, and noticed the exact same behavioral pattern repeating itself. His breaths were shallow and tightly controlled, as if deep, unrestricted breathing had been severely punished by someone in the past.
When the developed film came back from the darkroom, the broken ribs were clearly visible on the negative. There were two distinct fractures present. Crucially, the edges of the bone showed that the physical process of healing had already begun. This medical fact meant they could not possibly have been sustained during yesterday’s truck transport. They were significantly older.
Therefore, the boy had deliberately lied to the guards, or he was strictly repeating a prefabricated lie that he had been ordered to utilize by his superiors. But as the medic studied the glowing film against the light box, he perceived something else as well. It was not a clean, singular diagnosis or a simple, obvious answer. It was a broader pattern of trauma—a physical body that has been systematically damaged more than once, in more than one distinct way, over an extended period. And in a military prisoner of war camp that relies entirely on predictable routine, such a pattern represented a major disruption.
Returning to the main examination room, the medic did exactly what good, experienced clinicians do when faced with a traumatized patient. He actively worked to make the physical environment feel safer. He significantly lowered the volume of his voice, keeping his tone gentle and even. He maintained a calm, non-threatening posture, avoiding any sudden movements, and refused to rush the process. Then, he looked the boy directly in the eyes and spoke the specific words that mattered most.
“You are not in the German army anymore.”
The medic stepped closer.
“You are a prisoner of war now.”
He placed a reassuring hand near the cot.
“You are going to be properly fed, and you are going to be medically treated.”
He paused to let the words sink in.
“No one here is allowed to punish you for telling the truth.”
The boy swallowed hard, his throat muscles contracting. His eyes instantly flicked toward the heavy wooden door of the room. Even now, within the safety of an American medical facility, he fully expected someone to be listening through the wood, waiting to punish his compliance. The medic remained perfectly still, waiting patiently for the psychological tension to break. The boy finally opened his mouth to speak, and the very first thing that emerged from his lips was not a narrative about active military combat or battlefield tactics. It was an expression of pure, unadulterated fear.
“When you are young,” the boy began, his voice trembling slightly, “and the entire war is actively collapsing around you, fear is absolutely everywhere.”
He stared down at his hands.
“You feel fear of the enemy advancing, fear of the constant air attacks from above, fear of completely running out of food, and fear of being permanently separated from your unit.”
He paused, drawing a shallow, painful breath.
“But the worst fear of all is not always the enemy in front of you.”
He looked up at the medic, his eyes filled with a profound sadness.
“Sometimes, the worst fear is the men standing directly behind you.”
He stopped speaking again, carefully choosing each subsequent word as if it were a landmine that might explode if handled incorrectly. He began to explain that during the chaotic, frantic retreat across Western Europe, standard military discipline rapidly degenerated into raw, unchecked brutality. Orders were no longer spoken; they were screamed with frantic rage. Simple mistakes were never corrected through instruction; they were instantly punished with violence.
“If you fell behind the marching column,” the boy whispered, “you were immediately accused of cowardice.”
He tightened his grip on his uniform.
“If you complained about physical pain, you were accused of fatal weakness.”
He shook his head.
“If you asked for a moment of rest, you were accused of active sabotage.”
The boy was incredibly careful not to name specific individuals. He did not point blame at a single officer or sergeant. He spoke in the excessively cautious manner of someone who has deeply learned that the military system always finds a way to strike back against those who complain. He finally revealed that his ribs were broken during a severe beating. It was not the result of a single punch thrown in anger; it was inflicted by heavy combat boots, delivered via repeated, violent blows while he was lying helpless on the ground.
The medic felt a surge of intense anger rising within his own chest, but he forced his expression to remain entirely neutral. He knew that showing anger can easily cause a traumatized witness to shut down completely. Anger can make the boy retreat right back into his protective shell of absolute silence. Therefore, the medic asked the next logical question with extreme gentleness.
“Why were they beating you?”
The boy’s answer was incredibly quiet, barely audible over the hum of the building.
“Because I could not carry what they told me to carry.”
He looked at the floor.
“Because I was too weak.”
He swallowed.
“Because I slowed down the column.”
On the surface, that explanation should be more than enough to satisfy the inquiry. A collapsing army, rampant cruelty born of desperation, and sheer military panic—it all makes a grim kind of sense. But then the medic noticed the boy’s left hand slowly drifting toward his own right wrist. He began to rhythmically rub the skin there, moving his fingers as if he were remembering the painful pressure of a rope.
The medic leaned in closer to inspect the area. There were faint, distinct marks circling the wrists—half-healed abrasions, not fresh cuts, but older injuries. They are the exact kind of skin abrasions that come from being tightly bound with restraints, from being forcibly held down by multiple individuals, or from being deliberately forced to remain completely motionless for hours on end.
The boy suddenly realized that the medic had noticed his wrists. His eyes instantly tightened with panic, his mouth snapped shut, and a heavy, unresolved question now sat tangibly between them in the quiet room. Was this horrific treatment merely a case of excessively rough military discipline, or was it something infinitely worse?
The medic did not force the issue or press for an immediate answer. Instead, he strategically changed his angle of inquiry. He asked about his past food consumption.
“How much food were you eating before your capture?”
The boy answered far too quickly, his response almost automated.
“Not much.”
Then, he unexpectedly added a specific detail that did not fit the narrative of general wartime shortages.
“I had to give my bread to someone else.”
The medic immediately followed up.
“To who?”
The boy did not provide a name. Immediately, his throat moved sharply as he swallowed hard. He stared intently at the wooden floorboards and spoke in a low tone.
“To older men.”
He shifted his feet.
“To men with military rank.”
His voice dropped.
“To men who openly said they deserved it more than me.”
Now, the medic could clearly hear the true shape of the reality. This was not merely a standard story of frontline combat hardship. This was a story of a vulnerable youth being systematically consumed by a collapsing, predatory institution. And in that precise moment, the medic finally understood why the boy’s breathing remained so shallow, even when he was sitting perfectly still on the cot. It was not merely the physical pain of the fractures. It was a deeply ingrained habit. It was a survival reflex. Because when you are severely hurt and completely surrounded by desperate men who actively punish any sign of weakness, you quickly learn to hide the movement of your lungs.
The medic wrote far more extensive notes than usual on his chart. He was documenting the physical injuries, yes, but he was also meticulously documenting a broader pattern of systemic abuse that the standard military camp processing system is simply not designed to perceive. And the boy continued to watch every single mark made by the pencil, still deeply afraid that written words possess the power to hurt him.
Let us know in the comments where you’re watching this from. Are you in the United States, Germany, the United Kingdom, or somewhere else? We’d love to know who’s keeping these stories alive.
Now, back to the exam room, because the camp doctor is about to perform an action that surprises nearly everyone in the medical building. The senior camp doctor arrived with the calm, efficient speed of a medical officer who is deeply accustomed to handling daily emergencies. He carried a standard wooden clipboard, maintained a highly practiced, neutral professional expression, and operated under the initial assumption that this case would be entirely simple and routine. He expected to see broken ribs that required a standard cloth wrap, a prescription for bed rest, and a period of clinical observation.
But the medic stopped him before he entered, briefing him quietly in the hallway. He informed him of the two broken ribs that are already in the process of healing, the multiple distinct bruises scattered across the body in various stages of discoloration, the severe systemic weight loss, and the unmistakable restraint marks lining both wrists.
The doctor entered the room and looked directly at the boy, and the boy immediately looked away, refusing to meet his eyes. That single action told the experienced doctor an immense amount about his patient’s psychological state. People who have been consistently treated like human beings do not look away from a medical doctor by pure instinct.
The doctor began the physical examination from the very beginning, moving at a significantly slower, more deliberate pace. He checked the boy’s pulse rate; it was rapid and thready. He checked his body temperature and assessed his overall level of hydration. He carefully examined the interior of his mouth and gums, noting the classic clinical signs indicating that the physical body had been running on far too little nutrition for far too long.
Then, the doctor took an action that completely changed the psychological tone for everyone watching the interaction. He turned to the armed American guards standing by the doorway and asked them to step outside. It is a relatively small, simple order, but within a rigid prison environment, personal privacy represents immense power. The guards hesitated for a brief moment because they were strictly accustomed to being present during all prisoner interactions for security reasons. The doctor firmly insisted on his order. Finally, the heavy wooden door closed, and the guards’ footsteps receded.
Now, the room contained only the young boy, the medic, and the senior doctor. The doctor spoke in a completely plain, direct manner.
“You are safe enough to tell the truth here.”
He leaned in closer.
“If someone hurt you, say it.”
The boy’s face tightened instantly, his jaw clamping shut. He stared fixedly at the floorboards for a very long, heavy moment of silence. Then, he finally began to speak. And what emerged from his mouth was not a single, cohesive narrative. It consists of fractured fragments of memory. He spoke of a long, miserable road stretching through the pouring rain. He described a flatbed truck packed far too tight with desperate, shivering men. He talked about the acute shortage of daily food rations, an officer screaming hysterically about maintaining military discipline, a sudden, brutal kick delivered directly to his ribcage, and a long, freezing night where he could not lie down to rest because the simple act of breathing caused too much agony to bear.
The doctor listened intently, refusing to offer any interruptions. When the boy finally stops speaking, his breath ragged, the doctor asked one more critical question.
“Did this happen only once?”
The boy slowly shook his head from side to side.
“No.”
That single, quiet word delivered a profound shock to the medical staff. Because the camp administration fully expected the enemy to have injured him in battle. They expected standard battlefield trauma sustained from artillery shell fragments or bullet wounds. They did not expect a German teenager to arrive at their facility heavily injured by his own side, in a distinct manner that strongly suggests a pattern of repeated, systemic abuse.
The doctor made an immediate administrative decision. He ordered the boy to be officially admitted to the secure camp hospital area, even though medical space was incredibly tight due to the influx of prisoners. He prescribes a strict diet of soft, easily digestible foods. He ordered him to be placed on heavily restricted light work duty. He ordered regular, daily medical checks by the staff. Then, he looked directly at the medic and instructed him to document every single detail with extreme care, because thorough documentation represents their greatest shield. If anyone in the higher military command structures questioned why a single German prisoner is receiving such specialized, careful treatment, this medical record will become their legal protection.
When the armed guards were finally called back into the room, they looked at the doctor’s serious expression and immediately understood that something fundamental had shifted regarding this prisoner. They did not know the specific details of his confession. They only know that this particular boy is no longer considered just an anonymous number in a processing line.
The boy was carefully escorted over to a dedicated hospital cot. He moved with extreme slowness, keeping his arms held tightly against his torso, carefully guarding his fractured ribs. But for the very first time since he arrived at the camp, he stopped flinching at every sudden ambient sound. And that is the exact moment when the medic noticed another troubling detail. The boy was not only terrified of physical pain; he was deeply afraid of being seen by the other German prisoners in the compound. Because inside the barbed wire perimeter of a prison camp, the war does not always truly end. Sometimes, it continues to rage in low whispers, in dark acts of intimidation, and in the silent, brutal enforcement of old military rank and political ideology.
The question facing the medical staff became terrifyingly simple: if his own comrades violently injured him before his capture, what will happen to this boy if those exact same toxic dynamics follow him directly into the barracks?
In a standard United States prisoner of war camp, the heavy barbed-wire fences are designed to separate the captives from the guards. But inside the boundaries of the prisoner compound itself, an entirely different kind of separation can rapidly form. Old military ranks, old political loyalties, and old fears continue to hold sway over the men. Some of the prisoners continue to act as though the war is still actively raging on the outside. Some still behave as if their political ideology represents absolute law, and the younger, more vulnerable prisoners frequently become easy targets for their aggression—especially those who look physically weak, uncertain, or somehow different from the rest.
The medic began to observe these subtle dynamics very quickly. Whenever groups of German prisoners walked past the medical building, some glanced inside with calculating eyes, some deliberately look away, and a few stared for far too long with cold expressions. The boy noticed these looks as well. He immediately turned his face toward the wall whenever he heard footsteps passing by the window. He keeps his voice down to a bare whisper. He eats his food with frantic speed whenever a tray is brought to him, acting as though someone might step in and violently take it away at any moment.
The medic sat by his cot and asked him if there is anyone at all in the camp that he trusts—a friend from his old unit, a former bunkmate, or anyone he recognizes. The boy looked at him blankly and answered.
“No.”
He shifted beneath the blanket.
“I arrived entirely alone.”
He looked down.
“I was separated.”
That specific detail regarding his separation can mean many different things. Separation can be completely random, born of the chaos of war, or separation can be entirely deliberate. Sometimes, within the ranks of a collapsing army, the weak are intentionally pushed aside by their comrades. Sometimes, they are specifically selected for severe punishment. Sometimes, they are treated as a brutal public warning to the rest of the troops.
The medic became exceptionally careful now. He personally arranged the boy’s daily movements so that he was never forced to walk through crowded camp spaces alone. He scheduled his medical checks for times when the clinic was completely quiet and free of other patients. He did not announce any details of his condition in public, recognizing that the camp can be a safe environment, but only if that safety is built deliberately through constant vigilance.
Meanwhile, as the days passed, the boy’s physical body began to slowly heal. But true healing is not merely a matter of bone tissue knitting back together. Healing means learning that food will reliably arrive tomorrow. Healing means discovering that physical pain will be treated with medicine, rather than mocked with cruelty. Healing means learning that absolute silence is no longer the only way to survive.
One afternoon, the doctor examined the ribs once more. He pressed his fingers gently along the line of the fractures. The boy winced sharply from the pressure, but notably, he did not attempt to hide his discomfort. The doctor recognized this as genuine psychological progress. He asked the boy to describe how the injury occurred once more, not because he has forgotten the details, but because gentle repetition can often loosen the deeper truth.
This time, the boy added a specific detail that he had previously withheld. He explained that it occurred near a major rail yard during a highly chaotic retreat. He says a group of hungry soldiers had been accused of stealing military food rations. He says the punishments were carried out immediately on the spot, without any form of investigation or trial.
The medic listened closely, and something clicked in his mind. If the boy was merely accused, his ribs might not have been broken as a matter of standard military discipline alone. They might have been broken as an act of convenient scapegoating, as a piece of brutal public theater, as a horrific example designed to keep everyone else in the column completely obedient. That specific kind of institutional violence does not stop easily. It follows the survivors deep into their lives. It fundamentally shapes how they behave even in safe places, because to a traumatized mind, safe places always feel completely temporary.
And then, just as the boy begins to visibly relax into the routine of the clinic, a brand-new threat appears. He is officially scheduled to be moved out of the medical area and transferred back into the general barracks compound. It is a completely routine administrative move, but for him, it feels exactly like being violently sent back into the terrifying shadow he had barely escaped. He looks at the medic and asks a single question, his young voice cracking with emotion.
“Will they put me with the others?”
The medic asked him to clarify who he means. The boy refused to say it directly, choosing his words carefully.
“The ones who still think they can punish people.”
Now, the camp administrative staff faces a complex problem that no standard military manual solves easily. How do you protect a vulnerable prisoner from his fellow prisoners without causing a massive backlash that ultimately makes him even more vulnerable to their resentment?
In standard tales of wartime conflict, human suffering can easily become abstract until specific numbers pin it down to reality. The boy is exactly eighteen years old, which means he is barely older than many modern high school students. Yet, he is already carrying severe physical injuries that should belong to a much older veteran. Two of his ribs are completely broken, and because they are already in the process of healing, it means he lived through days or weeks of intense, agonizing pain with little to no real medical treatment while on the march.
Now, consider another number that matters immensely in prison camps like this: a single bunk assignment. That choice alone can completely determine whether a prisoner safely sleeps, eats, and heals, or whether he spends every single night bracing his body for physical intimidation. In a heavily crowded wooden barracks, it takes only a small handful of aggressive, ideologically driven men to force dozens of others to remain completely silent. The medic understands this reality deeply, even if nobody says it out loud, because discipline within a compound is not only what the external guards enforce. Sometimes, it is the brutal discipline that prisoners actively enforce on each other when they remain psychologically trapped in the rigid rules of the old world.
The camp doctor scheduled a meeting with the command staff. This is not a dramatic, emotional confrontation; it is handled as a highly practical, administrative conversation. The doctor explains that the boy requires continued, close medical monitoring. This clinical reality gives the command staff a perfectly legal and procedural reason to tightly control where the boy sleeps. They do not label it as protection on the official paperwork. Instead, they officially term it a matter of medical necessity. In a massive military bureaucracy, utilizing the correct wording can literally save a human life.
Consequently, the boy is placed in a specific barracks where the camp staff can see him much more easily during their rounds. He is assigned to much lighter daily duties. He is kept under steady observation long enough for his ribs to completely knit together and for his body weight to finally begin to recover. But the deeper, psychological recovery is a much slower process.
At night, the boy still wakes up shaking at any sudden ambient noise. He still startles violently whenever he hears heavy footsteps approaching his cot in the dark. He still eats his meals with frantic speed, as if the food might suddenly vanish if he looks away for a second. The medic attempts small, quiet kindnesses that do not embarrass him in front of the others—bringing him a second warm blanket when the nights turn freezing, offering an extra cup of clean water, and ensuring he has a quieter corner seat when official paperwork needs to be completed.
Over time, the boy begins to talk a little more, not in one large confession, but in small fragments that gradually form a clear pattern. He describes being rushed through a minimal training cycle because the front lines desperately needed physical bodies, not actual combat readiness. He describes older soldiers who were completely exhausted and filled with rage, consistently taking that anger out on the youngest replacements. He describes how pervasive fear turned ordinary men into ruthless predators, and how any sign of physical weakness became treated as a literal crime. Then, he utters a sentence that lands heavily on the medic’s mind.
“I was more afraid during the retreat than during my capture.”
That is not the sentence that people typically expect to hear from an enemy prisoner of war. But it makes perfect sense if the chaotic retreat is the exact place where his ribs were broken, where his food completely disappeared, and where the brutal punishments began. Capture for him did not represent a shameful defeat; it represented a definitive end to immediate terror. And that is the highly uncomfortable truth that deeply shocks the camp staff. Sometimes, the barbed-wire fence of a prison camp is not the first prison a person encounters. Sometimes, it is the second.
If you’re enjoying this story and want more untold accounts from World War II prisoners of war, make sure to subscribe to the channel. We’re bringing you stories that most history books never covered.
Now, listen closely to what happens when the boy finally enters the main camp routine, because the most dangerous moment is not the specific day he arrives. It is the day everyone stops actively watching him. As his fractured ribs continue to heal, the boy is officially cleared by the medical staff to leave the safety of the medical area more frequently. He walks at a noticeably slower pace than the other men, but he walks independently. He breathes much deeper now, though a sharp pain still catches him at the absolute edge of each deep inhalation.
The very first time he steps out into a busier section of the prisoner compound, the ambient conversations suddenly dip. This does not happen because he is famous or known to them; it occurs because visible vulnerability naturally draws attention in a harsh environment. The men see a boy with a slight limp, a boy who is far too thin, a boy who looks like he might be incredibly easy to dominate. He keeps his eyes fixed firmly on the ground. He wants absolutely no trouble, but trouble frequently finds the exact individuals who are trying the hardest to avoid it.
A sharp voice calls out something in German from directly behind him. The boy instantly stiffens, his posture freezing. The medic witnesses this interaction from a distance and feels his stomach tighten with anxiety. The boy does not respond to the call. He keeps walking forward. Another loud voice laughs mockingly.
He returns to the medical building that evening noticeably quieter than usual. His ribs did not receive any physical hits, and there are no new bruises on his skin, but the old, familiar fear is back in his eyes. The medic looks at him and asks a question.
“What happened?”
The boy answers with that single, familiar word.
“Nothing.”
That word nothing functions as a protective shield. It means that something definitely occurred, but he does not trust the administrative system to handle it safely. Or, he does not trust himself to survive the intense attention that an official complaint would bring upon him. The medic decides to change his strategy. Instead of pushing him for specific details, he asks a simple question.
“Do you feel safe in the barracks you will be assigned?”
The boy hesitates for a long moment, then slowly shakes his head. That response is more than enough for the staff. The medic takes the issue to the doctor again, and the doctor takes it directly to the command staff. The administrative solution remains exactly the same: not public punishment, not a dramatic spectacle, but the quiet, careful control of circumstances.
The boy is placed with a group of prisoners who are considered by staff to be significantly less likely to engage in bullying. He is kept close to the standard staff guard routes. He is kept on light duty assignments. He is monitored continuously without making the observation obvious to the population. To an outside observer, it would look like completely ordinary, boring camp administration. But to the boy, it feels like the very first time in his life that adults are utilizing authority to actively protect him, rather than break his spirit.
And slowly, over the passing days, his tense shoulders begin to drop. His breathing loosens. He begins to eat his meals at a normal, human pace. Then, on a quiet day when the rain taps softly against the tin roof of the clinic, he finally tells the medic the specific detail he has been hiding all this time. He explains that the severe beating which broke his ribs occurred after he explicitly refused to perform an action. It was not a refusal born of political rebellion; it was the refusal of a boy who still possessed a moral line that he simply would not cross. The medic looks at him and asks.
“What did they want you to do?”
The boy’s voice drops to an absolute whisper.
“They wanted me to accuse another soldier of theft.”
He swallows.
“A friend of mine. Someone younger, just like me.”
He looks up.
“I told them I would not do it.”
His voice trembles.
“I said I could not.”
And that is exactly when the heavy combat boots came. In that profound moment, the entire story becomes entirely clear to the medical staff. The broken ribs are not merely broken bones sustained in a chaotic war zone. They are tangible proof of a profound moral choice made under immense pressure, and viciously punished by men who desperately needed someone to blame. The medic writes the narrative down carefully in the record, not as a piece of medical drama, but as a permanent, factual record.
The boy does not transform into a conventional hero. There is no triumphant speech delivered to the camp, no dramatic cinematic revenge against his tormentors. There is only the quiet process of healing, day by day, in a place that remains a prison, but is no longer an active battlefield. His ribs mend sufficiently so that he can finally breathe deeply without wincing in pain. His body weight begins to steadily return. His eyes slowly lose some of their constant, anxious scanning.
And the camp staff learns a profound lesson that war frequently hides from view: not every single injury comes from the opposing enemy side. Not every prisoner arrives at a camp carrying only the physical damage of active combat. Some arrive carrying the deep, hidden damage of their own collapsing social and military system, the profound shame of what they witnessed, and the paralyzing fear that those terrors will follow them directly into captivity.
For the medic and the doctor, this specific case functions as a permanent reminder that a prisoner of war camp is not merely composed of wire fences and administrative rules. It is composed of human beings living in close proximity, carrying their past trauma along with them. And sometimes, the most critical work a camp staff can perform is not stopping escapes or enforcing rigid discipline. Sometimes, it is recognizing a boy who is still acting as though every single breath must be hidden from the world, and gently giving him a reason to breathe openly once again.
The real danger in an environment like this does not always announce itself with a loud shout. Sometimes, it arrives in the form of quiet laughter. Sometimes, it arrives in absolute silence. And sometimes, it arrives the exact moment the camp administration finally decides.
“You are well enough to be treated like everyone else.”
The boy’s broken ribs were healing well. His breathing was significantly deeper than it was on the day of his arrival. The senior doctor signed the official paperwork that officially cleared him to sleep in the general compound barracks once again. That single administrative decision should represent genuine clinical progress. But for the boy, it felt exactly like being violently pushed right back onto the same dangerous road where he was severely injured in the first place.
Because a medical cot possesses witnesses. A medical cot has established professional routines. A medical cot is surrounded by adults who can immediately intervene. A general barracks possesses dark shadows.
The medic walked alongside him across the wide compound at a slow, measured pace. The late afternoon sunlight filtered through the heavy barbed wire, striping the dirt ground like the bars of a cage. Men were sitting outside on their wooden bunks, writing letters home, mending old socks, or simply staring into nothingness. On the surface, the scene looks entirely calm, but that calmness can easily function as a mask that completely hides a brutal internal hierarchy.
Arriving at the barracks door, the medic paused. He spoke the boy’s name very softly, as if reminding him that he exists as an individual. The boy nodded his head, but his eyes were fixed intently on the dark interior of the room. He was actively scanning the faces, scanning the corners, scanning to see exactly who was standing up and who remained seated.
He stepped inside the threshold. The acoustic soundscape changed instantly. The sound of heavy boots on wooden floorboards echoed. Low, murmuring voices fill the air. A harsh cough echoed through the space. A man sitting near the center of the room looked up and stared at the boy for a second too long. The look was not overtly hostile, nor is it friendly; it was the cold, measuring gaze of a predator assessing prey.
The boy’s shoulders instantly tightened up. And the medic watched as the old, defensive reflex immediately returned to his body. Make yourself smaller. Make yourself entirely invisible. Do not draw any attention to yourself.
The boy’s specific bunk assignment was located near the very far end of the long room. That location was good in one sense: it meant significantly fewer people would brush past his bed during the day. But it was also bad in another sense: it means far fewer eyes will see exactly what occurs in that isolated corner at night.
That night, the boy lied down on his cot with extreme care. He attempted to sleep perfectly flat on his back because his ribs still ached with a dull pain whenever he tried to turn on his side. An American guard walked his patrol route outside the building. The sound of his footsteps gradually faded into the distance. Then, the wooden barracks became its own isolated world. Someone whispered a joke in the dark. Someone laughed quietly in response. A man told another man to move over on his mattress, utilizing far more physical force than was necessary. A wooden bunk creaked loudly as someone sat up in the dark.
The boy remained perfectly motionless. He forced his breathing to become shallow once again, even though he no longer had to from a medical standpoint. He had returned straight back to the old habit, the survival rule that dictates.
“Deep breathing makes noise, and noise brings unwanted eyes.”
A few bunks away, a low voice spoke in German. The tone was highly controlled and quiet, not a loud shout, but a firm command. The boy heard the voice and instantly stiffened in his bed because he recognized that exact tone. It is the identical tone that existed across the lines before his capture, back when military rank meant absolute power, and power meant you could violently hurt someone and call it discipline. And then, the psychological question becomes immediate and terrifying. Is that commanding voice coming for him tonight, or is it coming for someone else in the dark?
The following morning was not marked by dramatic violence. That absence of drama is exactly what made the environment so dangerous. The boy woke up and realized that no one had physically touched him during the night. There were no new bruises on his flesh, no open confrontations in the aisle. He should feel relaxed. Instead, he became significantly more alert and hyper-vigilant, because the torturous act of waiting for violence can often be far worse than the violence itself.
Standing in the morning mess hall line, he held his metal food tray tightly against his chest, as if physically guarding his torso. He ate his rations with frantic speed, keeping his eyes fixed downward, and the men standing around him noticed his behavior. One older German prisoner made a sharp comment in a quiet but cutting voice. He said something biting about the boy eating like a common thief.
The boy froze completely for a brief second, his spoon suspended, then he forced himself to keep eating. He had deeply memorized the primary rule of survival in a hostile environment. Do not react. Any visible reaction invites further escalation from bullies.
The medic encountered him later in the day and asked how his very first night in the general barracks went. The boy answered utilizing the exact same protective word he used before.
“Nothing.”
But the medic had learned to hear exactly what is hidden behind that word. Nothing can mean deep, paralyzing fear. Nothing can mean threats that were delivered too quietly to report to the guards. Nothing can mean a cruel lesson that was delivered entirely with threatening looks rather than physical fists. Therefore, the medic did not argue with him or press the issue. He asked a completely different question.
“Who did you sit next to at breakfast?”
The boy hesitated before answering, then named one specific man. It was a prisoner who said very little during the meal, who ate his food slowly, and who refused to participate in the cruel jokes of the others. The medic made a mental note of this detail. Inside a prisoner of war camp, alliances are not always based on genuine friendships. Sometimes, they are formed simply as shelter. Sometimes, they function as protection.
That evening, the medic purposefully invented an administrative excuse to walk past that specific barracks at the exact time the men were settling in for the night. He did not look directly at the boy’s corner, maintaining the appearance of a man performing routine safety checks. As he walked past the windows, he overhears a snippet of conversation in German. The discussion was about military rank. It was about who deserved to occupy the best bunks in the room. It was about who was truly brave on the front lines and who was inherently weak.
The boy remained perfectly quiet in his far corner, pretending to be completely oblivious to the talk, but the medic clearly saw his hand tighten firmly around the edge of his blanket. Then, someone in the room said something sharp that hits the boy’s ears like a physical slap. It was a line about traitors. It was a line about men who refuse to follow orders.
The boy’s head dipped noticeably lower toward his chest. He made his physical frame as small as humanly possible. Now, the medic fully understood the situation. The boy was not merely afraid of standard camp bullies. He was deeply terrified that someone in the barracks would discover the exact moral line he refused to cross back during the retreat, and violently punish him for it all over again. Because in that broken world, refusing to falsely accuse a friend can easily be framed as an act of treason. And disloyalty to the wrong group of desperate men is viewed as a crime worth beating out of you.
There is a constant temptation for the American camp staff to attempt to solve these complex problems with raw force—to physically separate the men, to severely punish any vocal threats, to make a grand public example of the agitators. But that direct approach can easily backfire inside the barbed wire. If you publicly punish the loudest men in the barracks, the internal violence simply becomes much quieter and harder to detect. If you move the victim out of the room in a highly public manner, the victim becomes permanently marked as an informant. And if you humiliate the wrong group of proud prisoners, their resentment grows exponentially.
Therefore, the senior doctor selected a much quieter, administrative solution. He met with the command staff and informed them that the boy’s fractured ribs require extended clinical monitoring. He formally recommended that the boy sleep in a bed located much closer to the medical clinic for strict medical reasons. The specific wording utilized in the report mattered immensely. Medical reasons sound entirely neutral to the prisoner population. Medical reasons do not cast blame or accuse anyone of a crime. Medical reasons do not spark a violent fight within the barracks.
And so, the boy was moved once again. The transfer was not executed with a dramatic spotlight, but with quiet paperwork. He received a different bunk in a different section of the camp, located a little closer to the watchful eyes of the staff. On the surface, it looks like standard, boring routine, but the boy understood exactly what it represented. It represented someone finally believing his fear without forcing him to prove it via a bloody confrontation in public.
That night, he slept for a significantly longer period—not perfectly, but longer than before. And in the morning, a small, quiet event occurred that the medic will remember for a very long time. The boy finished his breakfast in the mess hall, then purposefully left a thick piece of bread sitting on the edge of the wooden table. At first, the medic assumed the boy was simply full and cannot finish his ration. Then, he watched closely to see where the bread goes. It was quickly and quietly picked up by a much thinner prisoner, a man afflicted with a chronic cough who had been visibly struggling to survive the camp routine.
The boy did not look at the man. He did not make any public show of charity. He simply left the bread there and walked away. This act functioned as a quiet correction to the cruel world that had once violently forced him to surrender his own bread to men who claimed they deserved it more. That small act represented a major turning point—not a dramatic Hollywood moment, but a deeply human one. Because now, the boy was no longer merely surviving day to day; he is actively choosing exactly who he wants to be as a human being, even within the confines of captivity.
Just when the camp administration began to firmly believe that the crisis was completely over and the boy was safe, the medic noticed something during a routine physical check that made his blood run completely cold. It occurred during a standard inspection, a sudden glance when the boy lifted his arm to adjust his shirt. The medic spotted a distinct area of discoloration located near the upper arm. It looked exactly like a fresh bruise, bright and distinct from the faded yellow ones of his past beatings.
The medic asked about the mark in a casual, unconcerned tone. The boy answered far too quickly, his voice rising slightly.
“I bumped into a wooden bed frame.”
The medic did not openly challenge his statement. He gently asked to examine the area. The boy hesitated for a moment, then slowly revealed the skin. It was clearly not a bruise from a flat bed frame. It possessed the distinct, unmistakable shape of human fingers—a tight grip, a violent restraint.
Now, the medic possessed definitive physical confirmation that the boy’s fear was never imaginary. Something had occurred. It was not a massive beating or a loud riot; it was something highly controlled. It was a warning delivered in absolute quiet. The medic asked exactly where the incident occurred. The boy looked anxiously toward the door once again, his breathing catching. Then, he whispered his response.
“By the latrine line.”
He looked down.
“When the guards had their backs turned.”
The medic asked him to name who did it. The boy shook his head rapidly from side to side.
“I did not see.”
He gripped his shirt.
“It happened far too fast.”
He looked at the medic with pleading eyes.
“Please do not make it worse.”
That final, desperate line represents the absolute heart of prisoner survival in a hostile compound. Sometimes, the victim fears the long-term consequences of being protected far more than they fear the original physical threat, because institutional consequences can be endless.
So the camp staff chooses a different response. They institute a quiet, completely unannounced surveillance protocol covering the entire compound. Roving guards are assigned to walk random intervals near the latrine lines and back corners, effectively eliminating the blind spots where threats are quietly delivered. Rather than initiating a loud investigation that would mark the boy as a target, the command staff adjusts daily details, integrating the boy into administrative helper roles inside the safety of the main clinic building during peak hours.
Over the following months, the tight finger-shaped marks slowly fade from his skin, replaced by a healthier color as his rest and nutrition steadily improve. The medic continues to monitor him from across the processing desk, watching his movements become more fluid, less guarded. The boy’s breathing pattern gradually opens up, deep and regular. He no longer hides his lungs from the world. For the first time since stepping off the transport truck into the cloud of dust, he learns that the rules of authority can be used to safeguard a human life rather than break it, allowing him to finally outlive the terror of the men behind him.
Disclaimer : This content may be created by AI for entertainment purposes. Any resemblance to real persons, events, or places is coincidental.